

The Women’s Health Capital Thesis: Why Precision Health Is Becoming an Institutional Investment Opportunity
How sex-specific medicine, emerging healthcare LP demand, the Great Wealth Transfer, and specialist-manager access are reshaping women’s health investing.

Modern medicine was built on a contradiction.
It aimed to treat the human body. But for much of its history, the body it studied first and treated as the reference point was male.
That did not always mean women were absent from research. The deeper problem was that female biology was often treated as a variable to be excluded or controlled for, rather than a source of information to be understood.
As a result, treatments were developed with an incomplete picture of how sex and life stage might alter response. Symptoms that presented differently in women were missed and conditions that evolved differently across a woman’s life were diagnosed late.
The consequences run through the full arc of a woman’s life: from hormonal health to cardiovascular disease, autoimmune disease, brain health, bone health, mental health, cancer, chronic pain, and ageing.
But a new paradigm is emerging. It is being driven by the convergence of scientific progress, new diagnostic and data capabilities, ageing populations, and the rising cost of treating disease too late.
Its consequences will reach far beyond medicine. They will reshape how healthcare is designed, how risk is understood, and where capital looks for the next generation of growth.

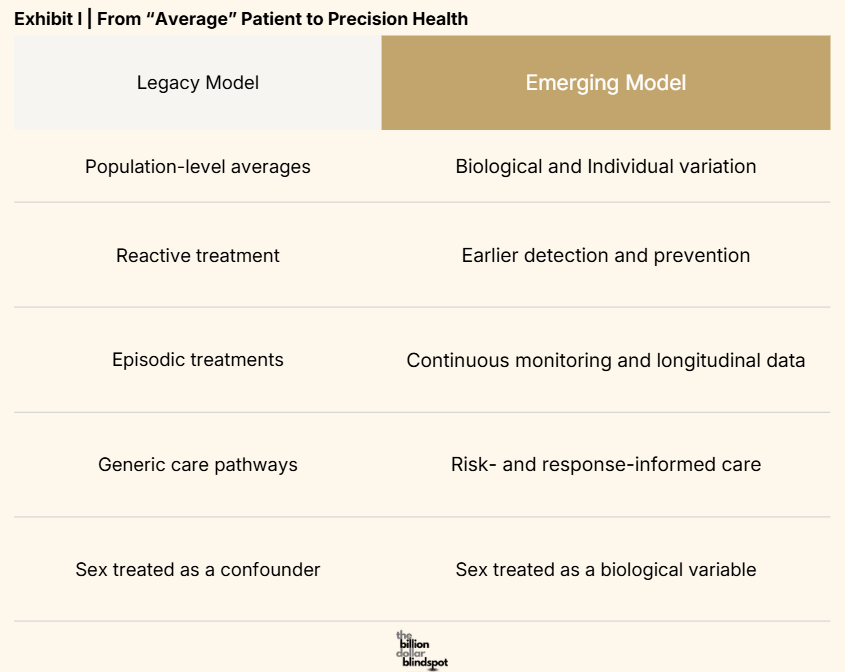
The old model of healthcare was built for a world of scarcity. Scarcity of data, diagnostic tools, computing power and longitudinal information about what happened to a person between one appointment and the next.
The practical response was to build systems around averages: standard pathways, broad populations, late intervention, and treatment after disease had already declared itself.
But that model is beginning to change. Genomics, biomarkers, more sensitive diagnostics, AI-enabled pattern recognition, wearables, remote monitoring, and new care-delivery models are making it possible to see disease earlier and with greater specificity. The ambition is no longer simply to treat a condition once it becomes obvious. It is to understand risk, monitor change, detect deviation, and intervene before a health problem becomes expensive, disabling, or irreversible.
This is what we mean by precision health—healthcare designed around the biological differences that determine who gets sick, how disease presents, what prevention looks like, and which treatment is most likely to work. Women’s health is one of the clearest tests of whether that transition is real.
Female biology affects disease risk, symptom presentation, progression, and treatment response across the life course.
Hormonal transitions can alter cardiovascular risk, bone density, cognition, metabolism, immune function, sleep, and mental health.
Pregnancy can reveal future cardiometabolic risk. Autoimmune disease disproportionately affects women. Chronic pain is more prevalent in women, yet has often been poorly understood and inadequately treated.
The National Institutes of Health now explicitly treats sex as a biological variable that should be considered in study design, analysis, and reporting. But policy recognition is not the same thing as full scientific integration. A recent National Academies review concluded that sex differences remain inconsistently implemented across research design and practice.
That gap is where the opportunity begins. When biology becomes more legible, markets once treated as peripheral become visible as infrastructure problems waiting to be solved.
Weekly capital intelligence on women's health, delivered directly to your inbox. Summer Special - 20% off. Offer ends June 30.
A New Class of LPs is Forming
The capital signal is already visible. Over the past several years, private capital has begun to look at women’s health differently. The conversation has moved beyond whether the category is “investable” at all.
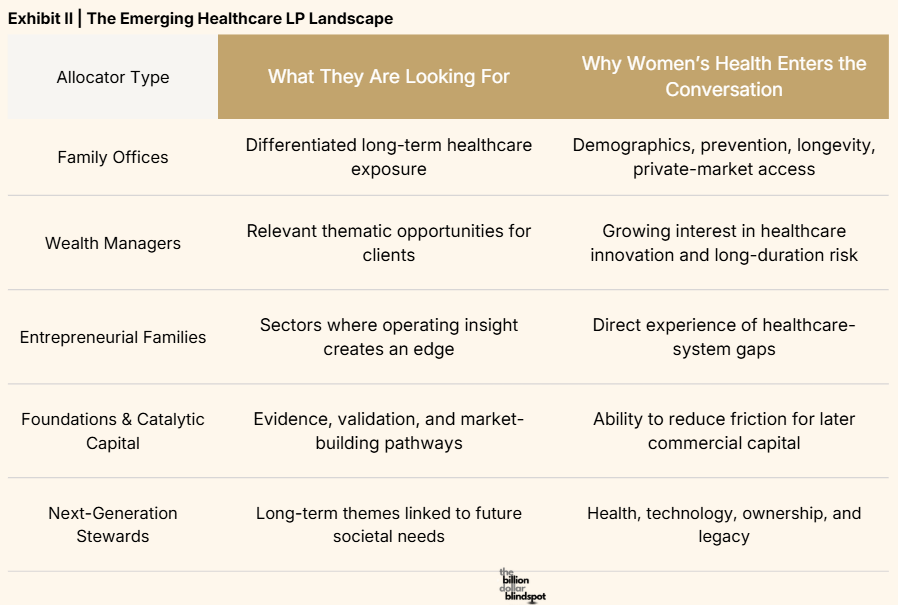
Increasingly, the questions are about access: which managers have real specialist expertise, where the strongest science is emerging, how to assess clinical and commercial maturity, and how to build exposure without reducing a global healthcare transition to one narrow theme. That shift is producing a new class of healthcare LPs.
It includes family offices looking for differentiated long-duration healthcare exposure; wealth managers responding to client interest in prevention, longevity, and healthcare innovation; entrepreneurial families with operating experience; healthcare executives; foundations; catalytic-capital providers; and next-generation capital stewards who see health not simply as a social issue, but as a structural economic one.
The Great Wealth Transfer which is currently ongoing through to the year 2048 matters here too. While the transfer of wealth to women does not mean that women who inherit or create wealth will automatically allocate to women’s health as capital decisions still remain shaped by mandate, risk appetite, family context, governance, and access.
But it does increase the number of people who hold, influence, or advise capital while also having direct experience of fertility care, pregnancy, chronic pain, menopause, caregiving, diagnostic delay, or the fragmented reality of healthcare systems.
This changes what they notice. It changes what they ask. It changes which questions reach private banks, family offices, investment committees, and advisers.
Investable before Institutionalisation
By now, the commercial case for women’s health is becoming harder to ignore.
There is growing scientific understanding. New companies are being built across diagnostics, therapeutics, care delivery, devices, data, and longevity. Private capital has begun to move into the category. And the underlying demand is not speculative: women are living longer, managing more chronic disease, and spending more years navigating healthcare systems that were not designed around their biology.
But recognition is not the same as access. A family office may see the opportunity and still struggle to answer a practical question: where, exactly, should we put capital to work?
That is because the category has developed faster than the infrastructure through which large pools of capital typically invest.
Institutional allocators typically invest through structures they can assess and govern: managers with long track records; vehicles that can absorb meaningfully sized tickets; benchmarks; portfolio-construction logic; and comparable data so that the opportunity can be evaluated alongside other healthcare allocations.
In women’s health, those structures are still emerging. This is not a reason to dismiss the category. It is a description of where the category sits in its development.
Climate investing offers a useful, limited parallel. The climate thesis was recognised before specialist managers, reporting standards, benchmarks, policy frameworks, and institutional familiarity had matured sufficiently for broad allocation. The thesis came first. The infrastructure followed. Capital scaled once it had credible routes through which to participate.
Women’s health is on a similar journey of capital formation, though not an identical one.
What the Biology Actually Does
The opportunity in women’s health is global, fragmented, and cross-disciplinary. It does not sit neatly inside one clinical category, one geography, one company type, or one investment stage. It stretches from diagnostics and therapeutics to care delivery, medical devices, data, ageing, and adjacent health technologies.
The expertise required to understand it is similarly dispersed. It often sits with specialist managers who have built relationships with founders, clinicians, researchers, hospitals, regulators, and local healthcare systems. These managers have developed the pattern recognition to identify a meaningful platform; the clinical networks to understand whether a therapy is genuinely differentiated; or the local knowledge to see where a care model can move from a promising service into durable infrastructure.
The strongest expertise is often held by these specialist managers that are relatively young in terms of track record, geographically dispersed, capacity constrained or too small for large institutional tickets. For larger allocators, that creates an access problem.
In this case, the answer is not simply to put more money into women’s health. The answer is to organise capital around specialist expertise: through disciplined manager selection, diversification across geography, clinical category, stage, and business model, governance, and institutional-quality portfolio construction.
The Question Capital Now Faces
Healthcare is becoming more precise. Private capital is beginning to seek exposure. The ownership and influence of wealth are changing. Yet the institutional architecture remains unfinished.
Women’s health is not a niche investment theme. It is where the transition to precision healthcare, the emergence of new healthcare LP demand, and the unfinished architecture of institutional capital meet.
The question is not whether this market will become more visible. It already is. The question is how we build credible routes for capital into the women’s health market.
Key takeaways
Women’s health is a core expression of the shift from average-based, reactive medicine to precision health: earlier detection, prevention, and care designed around biological variation.
Historical male-default research and insufficient analysis of sex differences have contributed to missed symptoms, delayed diagnosis, and incomplete treatment understanding across women’s lives.
The opportunity extends far beyond reproductive health: cardiovascular disease, autoimmune conditions, brain and bone health, mental health, cancer, chronic pain, pregnancy, ageing, diagnostics, and longevity.
A new class of healthcare LP is emerging as family offices, wealth managers, healthcare operators, foundations, and next-generation capital seek differentiated exposure to precision health and women’s health.
The Great Wealth Transfer is an accelerator, not the thesis: it broadens who holds and influences capital, but does not mean women will automatically invest in women’s health.
Women’s health is investable before it is fully institutionalised: innovation and demand are advancing faster than the manager scale, data, benchmarks, governance, and access routes required by large allocators.
The opportunity is global and fragmented; credible access requires specialist expertise, disciplined manager selection, diversification, and institutional-quality portfolio construction.
The Women’s Health Capital Thesis Map
Part I: The Women’s Health Capital Thesis — You are here
Part II: Why Women’s Health Is the First Test of Precision Health — Read Next
These questions sit at the heart of my new book, The Billion Dollar Blindspot. The book explores how outdated assumptions shaped research, innovation, and investment in women’s health and why some of the most important opportunities in healthcare may emerge when those assumptions begin to break down.
I’m grateful that the book recently reached #1 New Release on Amazon in its category, a sign that more readers are beginning to engage with these ideas. Because this conversation is ultimately about much more than menopause, hormones, or even women’s health.
It is about what happens when we finally start looking at the world as it is, rather than as it used to be. If you’d like to explore these ideas more deeply, you can find The Billion Dollar Blind Spot on Amazon.
References
National Academies of Sciences, Engineering, and Medicine, Review of NIH Structure, Policies, and Programs for Women’s Health Research (2025); NIH Office of Research on Women’s Health, NIH-Wide Strategic Plan for Research on the Health of Women 2024–2028.
Disclaimer & Disclosure
This content is for informational and educational purposes only. It does not constitute financial, investment, legal, or medical advice, or an offer to buy or sell any securities. Opinions expressed are those of the author and may not reflect the views of affiliated organisations. Readers should seek professional advice tailored to their individual circumstances before making investment decisions. Investing involves risk, including potential loss of principal. Past performance does not guarantee future results.